
Beliefs and Norms Associated with the Use of Ultra-Processed Commercial Milk Formulas for Pregnant Women in Vietnam

 ,
,  , , , , and
, , , , and 
Abstract
:1. Introduction
2. Methods
2.1. Study Design, Participants, Sampling, and Data Collection
2.2. Variables
2.2.1. Outcome Variables
2.2.2. Exposure Variables
2.2.3. Covariates
2.3. Data Analysis
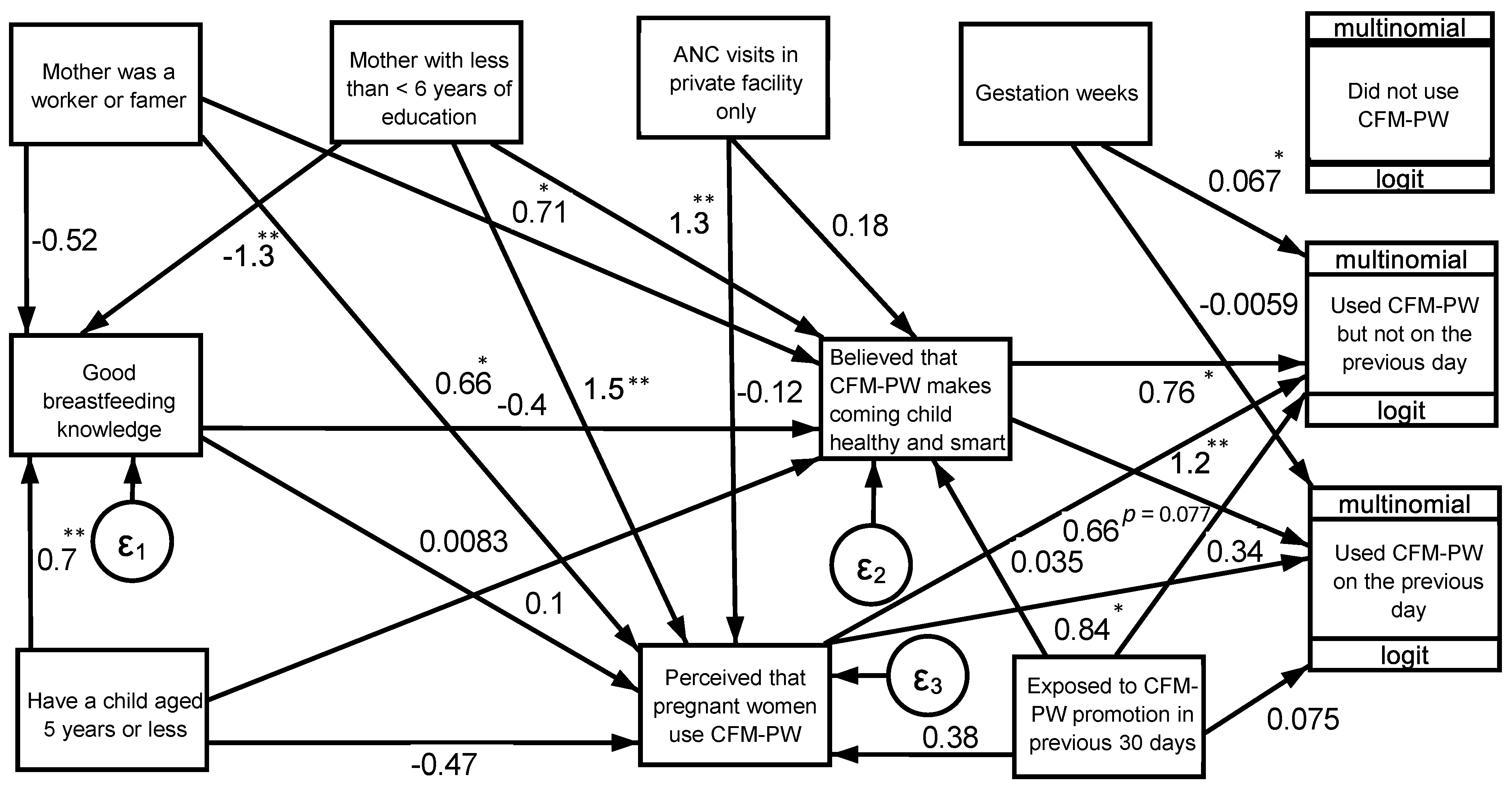
3. Results
4. Discussion
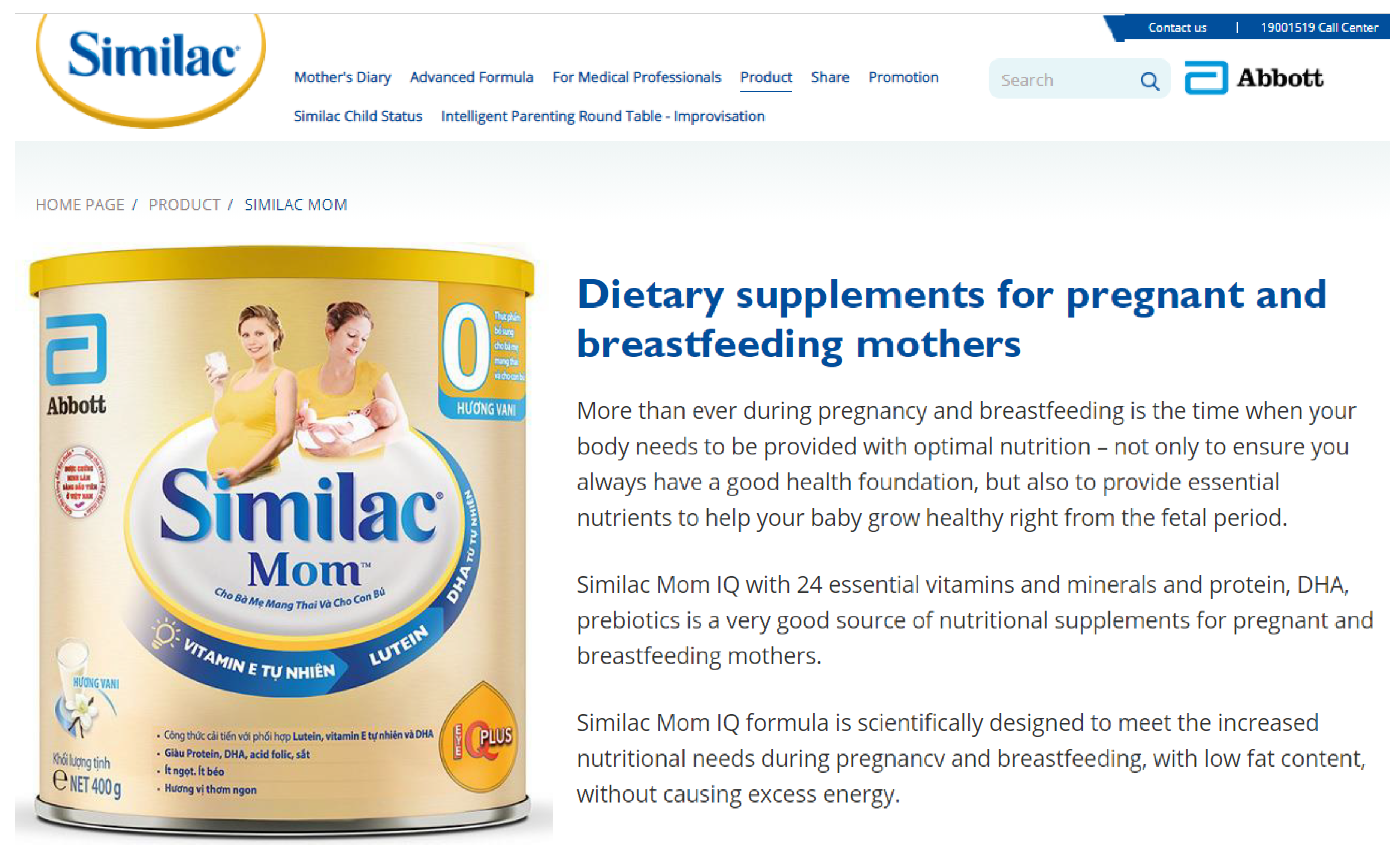
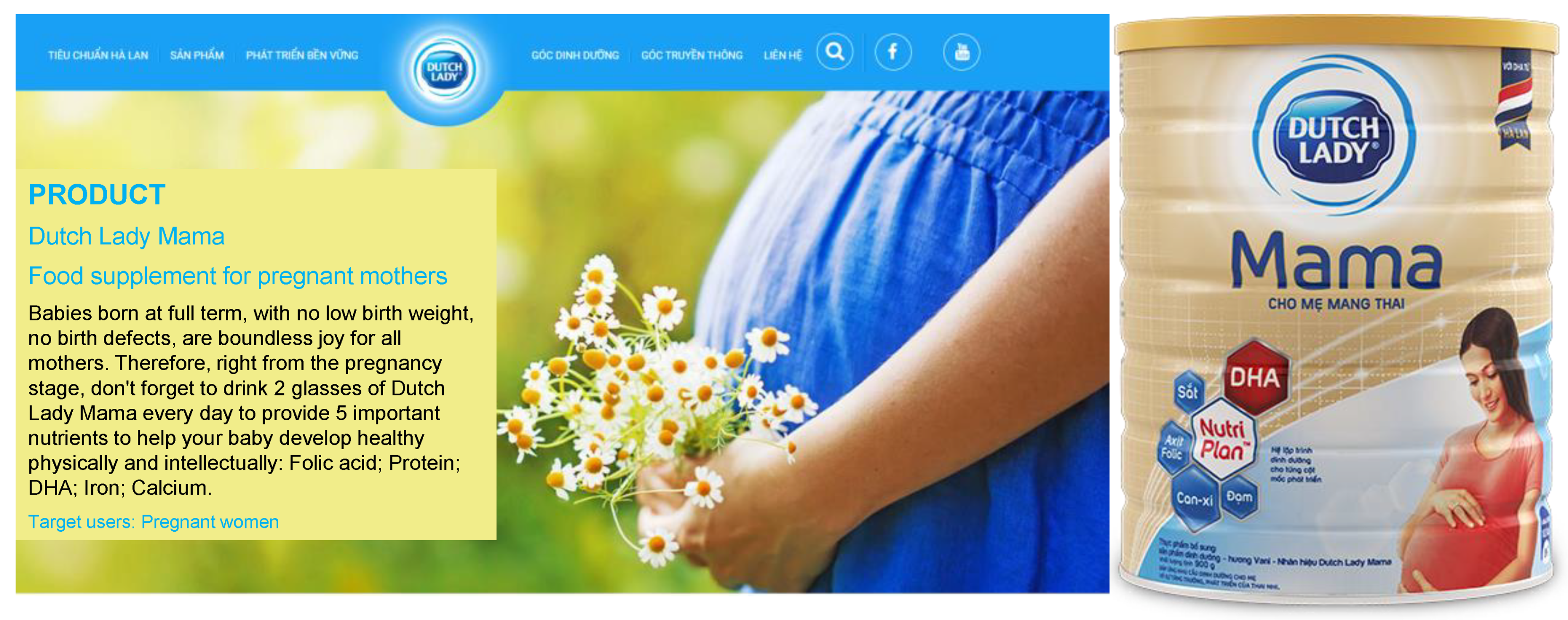
4.1. Promotional Messaging and Claims about the Benefits of CMF-PW
4.2. CMF Market Segmentation and Cross-Promotion Strategies
4.3. The CMF Industry Promotes CMF-PW with Approaches Prohibited under the Code
4.4. The CMF Industry Sponsors Research and Influences Health Policy
4.5. CMF-PW Promotion Should Be Better Regulated
4.6. Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Hinkle, S.N.; Schieve, L.A.; Stein, A.D.; Swan, D.W.; Ramakrishnan, U.; Sharma, A.J. Associations between maternal prepregnancy body mass index and child neurodevelopment at 2 years of age. Int. J. Obes. 2012, 36, 1312–1319. [Google Scholar] [CrossRef] [Green Version]
- Hinkle, S.N.; Sharma, A.J.; Swan, D.W.; Schieve, L.A.; Ramakrishnan, U.; Stein, A.D. Excess gestational weight gain is associated with child adiposity among mothers with normal and overweight prepregnancy weight status. J. Nutr. 2012, 142, 1851–1858. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Sharma, A.J.; Sappenfield, W.; Wilson, H.G.; Salihu, H.M. Association of maternal body mass index, excessive weight gain, and gestational diabetes mellitus with large-for-gestational-age births. Obstet. Gynecol. 2014, 123, 737–744. [Google Scholar] [CrossRef]
- Development Initiatives. Global Nutrition Report 2020: Action on Equity to End Malnutrition; Development Initiatives: Bristol, UK, 2020. [Google Scholar]
- Development Initiatives. Global Nutrition Report 2018: Shining a Light to Spur Action on Nutrition; Development Initiatives: Bristol, UK, 2018. [Google Scholar]
- Magnant, C. The nutritional market for pregnant and breastfeeding women: What opportunities are there for dairy ingredients? In Lactalis Ingredients; Lactalis Ingredients: Bourgbarré, France, 2021. [Google Scholar]
- Abbott. Similac Mom IQEye: Dietary Supplements for Pregnant and Breastfeeding Mothers. Available online: https://similac.com.vn/san-pham/similac-mom (accessed on 20 August 2021).
- Baker, P.; Russ, K.; Kang, M.; Santos, T.M.; Neves, P.A.R.; Smith, J.; Kingston, G.; Mialon, M.; Lawrence, M.; Wood, B.; et al. Globalization, first-foods systems transformations and corporate power: A synthesis of literature and data on the market and political practices of the transnational baby food industry. Glob. Health 2021, 17, 58. [Google Scholar] [CrossRef] [PubMed]
- Hastings, G.; Angus, K.; Eadie, D.; Hunt, K. Selling second best: How infant formula marketing works. Glob. Health 2020, 16, 77. [Google Scholar] [CrossRef] [PubMed]
- Piwoz, E.G.; Huffman, S.L. The Impact of Marketing of Breast-Milk Substitutes on WHO-Recommended Breastfeeding Practices. Food Nutr. Bull. 2015, 36, 373–386. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.; Weissman, A.; Cashin, J.; Ha, T.T.; Zambrano, P.; Mathisen, R. Assessing the Effectiveness of Policies Relating to Breastfeeding Promotion, Protection, and Support in Southeast Asia: Protocol for a Mixed Methods Study. JMIR Res. Protoc. 2020, 9, e21286. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.; Tran, H.T.T.; Cashin, J.; Nguyen, V.D.C.; Weissman, A.; Nguyen, T.T.; Kelly, B.; Mathisen, R. Implementation of the Code of Marketing of Breast-Milk Substitutes in Vietnam: Marketing Practices by the Industry and Perceptions of Caregivers and Health Workers. Nutrients 2021, 13, 2884. [Google Scholar] [CrossRef]
- Vietnam National Institute of Nutrition. Breastfeeding–Strategy for Combating Malnutrition. Available online: http://viendinhduong.vn/vi/dinh-duong-tre-em/nuoi-con-bang-sua-me-giai-phap-phong-chong-suy-dinh-duong-nhan-tuan-le-nuoi-con-bang-sua-me-tu-18-782015.html (accessed on 25 September 2021).
- Dehejia, R.H.; Wahba, S. Propensity Score-Matching Methods for Nonexperimental Causal Studies. Rev. Econ. Stat. 2002, 84, 151–161. [Google Scholar] [CrossRef] [Green Version]
- Mejia, P.; Seklir, L.; Gardin, K.; Nixon, L. Mother and Child Promotion: A Preliminary Analysis of Social Media Marketing of Infant Formula; Berkeley Media Studies Group: Berkeley CA, USA, 2016. [Google Scholar]
- Berry, N.J.; Jones, S.C.; Iverson, D. Circumventing the WHO Code? An observational study. Arch. Dis. Child. 2012, 97, 320–325. [Google Scholar] [CrossRef] [Green Version]
- Berry, N.J.; Jones, S.; Iverson, D. It’s all formula to me: Women’s understandings of toddler milk ads. Breastfeed. Rev. 2010, 18, 21–30. [Google Scholar]
- Pharmacy365. The Top 10 Milks for Pregnant Women in the First 3 Months. Available online: https://nhathuoc365.vn/top-5-loai-sua-an-thai-danh-rieng-cho-ba-bau-3-thang-dau-nd1764 (accessed on 20 August 2021).
- FrieslandCampina. Dutch Lady Mama: Dietary Supplements for Pregnant Women. Available online: https://www.dutchlady.com.vn/san-pham/sua-me-mama (accessed on 20 August 2021).
- Vinamilk. Dielac Mama Gold: Healthy Moms, Smart Babies. Available online: https://www.vinamilk.com.vn/sua-bot-vinamilk/en/product/dielac-mama-en/ (accessed on 20 August 2021).
- VitaDairy. ColosBaby Gold for Mum. Available online: https://vitadairy.vn/en/products/product-for-mums/colosbaby-gold-for-mum (accessed on 26 August 2021).
- Vietnam Government. Decree 100/2014/NĐ-CP on the Trading in and Use of Nutritious Products for Infants, Feeding Bottles and Teats; Vietnam Government: Hanoi, Vietnam, 2014.
- Pereira, C.; Ford, R.; Feeley, A.B.; Sweet, L.; Badham, J.; Zehner, E. Cross-sectional survey shows that follow-up formula and growing-up milks are labelled similarly to infant formula in four low and middle income countries. Matern. Child Nutr. 2016, 12 (Suppl. S2), 91–105. [Google Scholar] [CrossRef]
- Cattaneo, A.; Pani, P.; Carletti, C.; Guidetti, M.; Mutti, V.; Guidetti, C.; Knowles, A.; Follow-on Formula Research Group. Advertisements of follow-on formula and their perception by pregnant women and mothers in Italy. Arch. Dis. Child. 2015, 100, 323–328. [Google Scholar] [CrossRef]
- IBFAN-ICDC. Annotated Compilation of the International Code of Marketing of Breastmilk Substitutes and Relevant WHA Resolutions (Updated in 2018); IBFAN-ICDC: Penang, Malaysia, 2018. [Google Scholar]
- MeadJohnson Nutrition. Products from Enfa+. Available online: https://www.enfa.com.vn/san-pham/sua-cho-me-mang-thai-va-cho-con-bu (accessed on 20 August 2021).
- Berry, N.J.; Jones, S.C.; Iverson, D. Toddler Milk Advertising in Australia: Infant Formula Advertising in Disguise? Australas. Mark. J. 2021, 20, 24–27. [Google Scholar] [CrossRef]
- WHO. Guidance on Ending the Inappropriate Promotion of Foods for Infants and Young Children: Implementation Manual; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Zhang, Z.; Tran, N.T.; Nguyen, T.S.; Nguyen, L.T.; Berde, Y.; Tey, S.L.; Low, Y.L.; Huynh, D.T.T. Impact of maternal nutritional supplementation in conjunction with a breastfeeding support program during the last trimester to 12 weeks postpartum on breastfeeding practices and child development at 30 months old. PLoS ONE 2018, 13, e0200519. [Google Scholar] [CrossRef] [Green Version]
- Huynh, D.T.T.; Tran, N.T.; Nguyen, L.T.; Berde, Y.; Low, Y.L. Impact of maternal nutritional supplementation in conjunction with a breastfeeding support program on breastfeeding performance, birth, and growth outcomes in a Vietnamese population. J. Matern. Fetal Neonatal Med. 2018, 31, 1586–1594. [Google Scholar] [CrossRef] [PubMed]
- Tran, N.T.; Nguyen, L.T.; Berde, Y.; Low, Y.L.; Tey, S.L.; Huynh, D.T.T. Maternal nutritional adequacy and gestational weight gain and their associations with birth outcomes among Vietnamese women. BMC Pregnancy Childbirth 2019, 19, 468. [Google Scholar] [CrossRef]
- Vietnam Ministry of Health. National Guideline on Nutrition for Pregnant Women and Lactating Mothers in 776/QĐ-BYT; Vietnam Ministry of Health: Hanoi, Vietnam, 2017.
- WHO. International Code of Marketing of Breast-milk Substitutes; World Health Organization: Geneva, Switzerland, 1981. [Google Scholar]
- Grummer-Strawn, L.M.; Holliday, F.; Jungo, K.T.; Rollins, N. Sponsorship of national and regional professional paediatrics associations by companies that make breast-milk substitutes: Evidence from a review of official websites. BMJ Open 2019, 9, e029035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Son, N.T.; Barraclough, S.; Morrow, M.; Trung, D.Q. Controlling infant formula promotion in Ho Chi Minh City, Vietnam: Barriers to policy implementation in the health sector. Aust. J. Prim. Health 2000, 6, 27–36. [Google Scholar]
- WHO. Healthy Eating During Pregnancy and Breastfeeding: Booklet for Mothers; WHO Regional Office for Europe: Copenhagen, Denmark, 2001. [Google Scholar]
- Kominiarek, M.A.; Rajan, P. Nutrition Recommendations in Pregnancy and Lactation. Med. Clin. N. Am. 2016, 100, 1199–1215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centre for Clinical Practice at NICE. Maternal and Child Nutrition; Centre for Clinical Practice at NICE: London, UK, 2014. [Google Scholar]
- Homer, C.S.; Oats, J.; Middleton, P.; Ramson, J.; Diplock, S. Updated clinical practice guidelines on pregnancy care. Med. J. Aust. 2018, 209, 409–412. [Google Scholar] [CrossRef] [PubMed]
- Caut, C.; Leach, M.; Steel, A. Dietary guideline adherence during preconception and pregnancy: A systematic review. Matern. Child. Nutr. 2020, 16, e12916. [Google Scholar] [CrossRef] [Green Version]
- Jouanne, M.; Oddoux, S.; Noel, A.; Voisin-Chiret, A.S. Nutrient Requirements during Pregnancy and Lactation. Nutrients 2021, 13, 692. [Google Scholar] [CrossRef]
- Achon, M.; Ubeda, N.; Garcia-Gonzalez, A.; Partearroyo, T.; Varela-Moreiras, G. Effects of Milk and Dairy Product Consumption on Pregnancy and Lactation Outcomes: A Systematic Review. Adv. Nutr. 2019, 10, S74–S87. [Google Scholar] [CrossRef]
- Brantsaeter, A.L.; Olafsdottir, A.S.; Forsum, E.; Olsen, S.F.; Thorsdottir, I. Does milk and dairy consumption during pregnancy influence fetal growth and infant birthweight? A systematic literature review. Food Nutr. Res. 2012, 56, 20050. [Google Scholar] [CrossRef] [Green Version]
- Murphy, E.G.; Regost, N.E.; Roos, Y.H.; Fenelon, M.A. Powder and Reconstituted Properties of Commercial Infant and Follow-On Formulas. Foods 2020, 9, 84. [Google Scholar] [CrossRef] [Green Version]
- Masum, A.K.M.; Chandrapala, J.; Huppertz, T.; Adhikari, B.; Zisu, B. Production and characterization of infant milk formula powders: A review. Dry. Technol. 2020, 39, 1492–1512. [Google Scholar] [CrossRef]
- Rotronic. Milk Powder Production. Available online: https://www.rotronic.com/en-us/rotronic-cases-read?id=364/ (accessed on 29 July 2021).
- Belitz, H.D.; Grosch, W.; Schieberle, P. Food Chemistry; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.C.; Louzada, M.L.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; et al. Ultra-processed foods: What they are and how to identify them. Public Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Ballard, O.; Morrow, A.L. Human milk composition: Nutrients and bioactive factors. Pediatr. Clin. N. Am. 2013, 60, 49–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cerbulis, J.; Farrell, H.M., Jr. Composition of milks of dairy cattle. I. Protein, lactose, and fat contents and distribution of protein fraction. J. Dairy Sci. 1975, 58, 817–827. [Google Scholar] [CrossRef]
- Coca-Cola. Classic Coca-Cola: Nutrition. Available online: https://www.coca-colacompany.com/au/brands/coca-cola#contentwrapper1 (accessed on 20 August 2021).
- WHO. Guideline: Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Buyken, A.E.; Mela, D.J.; Dussort, P.; Johnson, I.T.; Macdonald, I.A.; Stowell, J.D.; Brouns, F. Dietary carbohydrates: A review of international recommendations and the methods used to derive them. Eur. J. Clin. Nutr. 2018, 72, 1625–1643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mustafa, S.T.; Hofer, O.J.; Harding, J.E.; Wall, C.R.; Crowther, C.A. Dietary recommendations for women with gestational diabetes mellitus: A systematic review of clinical practice guidelines. Nutr. Rev. 2021, 79, 988–1021. [Google Scholar] [CrossRef] [PubMed]
- Rohatgi, K.W.; Tinius, R.A.; Cade, W.T.; Steele, E.M.; Cahill, A.G.; Parra, D.C. Relationships between consumption of ultra-processed foods, gestational weight gain and neonatal outcomes in a sample of US pregnant women. PeerJ 2017, 5, e4091. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Estimates (n = 268) | |
|---|---|
| Kinh ethnicity | 93.3 |
| Age (Mean ± SD; Median (p25–p75)) | 29.3 ± 5.9 29 (25–33) |
| Married | 99.3 |
| Living with partners | 96.3 |
| Highest level of education: | |
| Primary school or less | 17.5 |
| Junior secondary school | 24.3 |
| Secondary school | 23.1 |
| Some college or higher | 35.1 |
| Main occupations: | |
| Blue-collar or farmer | 19.4 |
| White-collar | 21.6 |
| Small trader, self-employed, small self-owned business, services | 34 |
| Unemployed, homemaker, student | 25 |
| Estimates (n = 268) | |
|---|---|
| Use of CMF-PW: | |
| Have not used | 35.4 |
| Have used, but not on the previous day | 29.9 |
| Used on the previous day | 34.7 |
| Believed that CMF-PW makes a child smart and healthy 2 | 53.7 |
| Perceived that most pregnant women use CMF-PW 2 | 70.9 |
| Exposed to promotion of CMF-PW in the previous 30 days | 23.9 |
| Ever contacted by CMF industry representative during ANC visit | 18.3 |
| Breastfeeding knowledge: | |
| Breastfeeding knowledge score 3 (Mean ± SD; Median (p25–p75)) | 1.9 ± 0.9 2 (1–3) |
| No correct responses | 4.9 |
| Correct response to 1 question | 25.4 |
| Correct response to 2 questions | 40.7 |
| Correct response to all 3 questions | 29.1 |
| Estimates (n = 268) | |
|---|---|
| Location of ANC: | |
| Public health facilities only | 21.3 |
| Both public and private health facilities | 27.2 |
| Private health facilities only | 51.5 |
| Gestation weeks (Mean ± SD; Median (p25–p75)) | 25.7 ± 7.6 26.8 (20.9–32.0) |
| In 3rd trimester | 43.7 |
| Number of ANC visits (Mean ± SD; Median (p25–p75)) | 4.2 ± 3.4 3.5 (2–6) |
| Had a child aged 5 years or less | 44.0 |
| Occasional Consumption | Recent Consumption | |
|---|---|---|
| Believed that CMF-PW makes a child smart and healthy 2 | 1.94 (0.9, 4.2) | 3.56 ** (1.65, 7.71) |
| Perceived that most pregnant women use CMF-PW 2 | 1.69 (0.76, 3.78) | 2.29 * (1.13, 4.66) |
| Breastfeeding knowledge score 3 | 1.17 (0.74, 1.85) | 1.22 (0.82, 1.83) |
| Exposed to promotion of CMF-PW in the previous 30 days | 1.77 (0.77, 4.07) | 0.99 (0.45, 2.17) |
| Location of ANC: | ||
| Public health facilities | 1 (1, 1) | 1 (1, 1) |
| Both public and private health facilities | 1.17 (0.42, 3.24) | 1.28 (0.52, 3.13) |
| Private health facilities | 1.43 (0.59, 3.51) | 0.84 (0.42, 1.67) |
| Ever contacted by CMF industry representative during ANC visit | 1.2 (0.49, 2.93) | 2.02 (0.82, 4.98) |
| Gestation weeks | 0.91 (0.81, 1.02) | 0.99 (0.89, 1.09) |
| Number of ANC visits | 1.09 ** (1.03, 1.16) | 0.99 (0.95, 1.03) |
| Had a child aged 5 years or less | 0.54 (0.28, 1.03) | 0.85 (0.42, 1.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, T.T.; Cashin, J.; Ching, C.; Baker, P.; Tran, H.T.; Weissman, A.; Nguyen, T.T.; Mathisen, R. Beliefs and Norms Associated with the Use of Ultra-Processed Commercial Milk Formulas for Pregnant Women in Vietnam. Nutrients 2021, 13, 4143. https://doi.org/10.3390/nu13114143
Nguyen TT, Cashin J, Ching C, Baker P, Tran HT, Weissman A, Nguyen TT, Mathisen R. Beliefs and Norms Associated with the Use of Ultra-Processed Commercial Milk Formulas for Pregnant Women in Vietnam. Nutrients. 2021; 13(11):4143. https://doi.org/10.3390/nu13114143
Chicago/Turabian StyleNguyen, Tuan T., Jennifer Cashin, Constance Ching, Phillip Baker, Hoang T. Tran, Amy Weissman, Thao T. Nguyen, and Roger Mathisen. 2021. "Beliefs and Norms Associated with the Use of Ultra-Processed Commercial Milk Formulas for Pregnant Women in Vietnam" Nutrients 13, no. 11: 4143. https://doi.org/10.3390/nu13114143