Article Text

Abstract
Introduction Automated insulin delivery (also known as closed loop, or artificial pancreas) has shown potential to improve glycaemic control and quality of life in people with type 1 diabetes (T1D). Automated insulin delivery devices incorporate an insulin pump with continuous glucose monitoring(CGM) and an algorithm, and adjust insulin in real time. This study aims to establish the safety and efficacy of a hybrid closed-loop (HCL) system in a long-term outpatient trial in people with T1D aged 12 –<25 years of age, and compare outcomes with standard therapy for T1D as used in the contemporary community.
Methods and analysis This is an open-label, multicentre, 6-month, randomised controlled home trial to test the MiniMed Medtronic 670G system (HCL) in people with T1D aged 12 –<25 years, and compare it to standard care (multiple daily injections or continuous subcutaneous insulin infusion (CSII), with or without CGM). Following a run-in period including diabetes and carbohydrate counting education, dosage optimisation and baseline glucose control data collection, participants are randomised to either HCL or to continue on their current treatment regimen. The primary aim of the study is to compare the proportion of time spent in target sensor glucose range (3.9–10.0 mmol/L) on HCL versus standard therapy. Secondary aims include a range of glucose control parameters, psychosocial measures, health economic measures, biomarker status, user/technology interactions and healthcare professional expectations. Analysis will be intention to treat. A study in adults with an aligned design is being conducted in parallel to this trial.
Ethics and dissemination Ethics committee permissions were gained from respective institutional review boards. The findings of the study will provide high-quality evidence on the role of HCL in clinical practice.
- clinical trials
- paediatrics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This a long-term outpatient randomised controlled home trial in people aged 12 –<25 years of age with type 1 diabetes (T1D) comparing a hybrid closed-loop (HCL) system to standard care.
The secondary objectives are wide in scope, and will provide a full evaluation of the clinical application of HCL technology for people with T1D.
This study of people with diabetes aged 12–<25 years has glucose end-points aligned with a concurrent study examining HCL in adults >25 years old, thereby facilitating comparison of metabolic outcomes between these two populations.
The technology is rapidly evolving, and results of this study may underestimate the future potential of automated insulin delivery systems.
Introduction
Automated insulin delivery (also known as closed loop or ‘artificial pancreas’) systems consist of an insulin pump (CSII), a continuous glucose monitor (CGM) and an algorithm that determines the automated insulin delivery. Single (insulin only) and dual (insulin and glucagon) systems have been developed. A variety of platforms exist using different combinations of insulin pumps, CGM and algorithms (there are three core algorithm constructs: (1) proportional integrative derivative (PID),1 (2) model predictive control2 and (3) fuzzy logic3). Hybrid closed-loop (HCL) systems use the algorithm to control background (or basal) insulin requirements while meal announcement with carbohydrate estimation and bolusing are still required to be entered manually by the user. The technical evolution in automated insulin delivery has been rapid, from proof of concept experiments in 20064 to the first commercial release of a single hormone hybrid system (MiniMed 670G, USA only, approved for those aged 14 years and over) in 2017.
The development of automated insulin delivery has been driven by the goal of achieving improved time spent in target glucose range, while minimising hypoglycaemia. Long-term poor control is known to predict the development of diabetes complications.5 However, despite improvements in diabetes education, insulin pharmacology, glucose monitoring and insulin delivery devices, fewer than a third of patients reach haemoglobin A1c (HbA1c) targets set by international guidelines.6 Further, adolescence and young adulthood are particularly high-risk age groups, during which glycaemic control is at its poorest.6 The burden of managing diabetes is high for the patient and their caregivers, resulting in poor quality of life7 and high rates of psychological comorbidity.8 Automated insulin delivery has the potential to improve glycaemic control and improve quality of life during this vulnerable period.
Due to the complex care required, development of complications and loss of productivity, type 1 diabetes (T1D) incurs a significant burden on healthcare budgets. In Australia, it is estimated that $A200 million per annum is spent on T1D.9 As the incidence of T1D is increasing,10 11 new approaches like automated insulin delivery are required to improve patient outcomes, and have the potential to reduce the economic impact.
To date, several outpatient studies using automated insulin delivery have been published. Although heterogeneous in design and with a variety of automated and semiautomated insulin±glucagon delivery systems employed, a meta-analysis of studies that were conducted at home, camps and in hotels demonstrated a 12.59% overall improvement in time spent in target range (3.9–10.0 mmol/L) when compared with standard insulin pump therapy (CSII) or sensor-augmented pump (SAP) therapy.12 The longest duration of follow-up for included studies was 12 weeks.13 This included two substudies: (1) a study in adults (n=33) who used the system 24 hours per day, and (2) a study in children and adolescents (n=25) who used the system overnight. Adults improved time in target range (3.9–10.0 mmol/L) by 11%, and the children and adolescents improved overnight glucose time in target range (3.9–8.0 mmol/L) by 24.7%.13 There are other large long-term multisite trials investigating closed-loop technology currently underway.
The only automated insulin delivery device that is currently commercially available is the MiniMed 670G, although only available in the USA and approved for people with T1DM aged above 14 years. A non-controlled pivotal safety study using this device in patients aged 14–75 years (n=124) for 3 months demonstrated safety; in addition, diabetes control was improved and HbA1c reduced from 7.4% to 6.9%.14 Adolescent participants used the automated insulin delivery feature (‘Auto Mode’) 75.8% of the time and demonstrated a change in HbA1c from 7.7%±0.8% to 7.1%±0.6%.15
Longer duration and controlled studies are required to quantify efficacy of the MiniMed 670G system. Our study is a 6-month multisite randomised controlled study that compares the Medtronic 670G system to standard therapy (CSII or multiple daily injections (MDI), with or without CGM). We will assess the impact on glucose control and quality of life, and conduct health economic analyses.
We hypothesise that the HCL MiniMed 670G system (HCL hereinafter) will improve the time spent in target glucose range by 7% compared with standard therapy (CSII or MDI, with or without CGM). We further hypothesise that HCL will reduce hypoglycaemia (time spent <3.9 mmol/L) by 60%. A number of other glucose control metrics (time spent in high glucose range, glucose variability, night-time glucose, daytime glucose) are hypothesised to improve, as well as quality of life measurements.
Aims
The primary objective of the study is to compare the proportion of time that sensor glucose is in target range (3.9–10.0 mmol/L) using HCL versus standard therapy (CSII, MDI, with or without CGM), measured by masked CGM at 23–26 weeks post randomisation. The primary objective and secondary objectives are listed in table 1.
Primary and secondary objectives
Biomarkers
Cell adhesion molecules (CAM)S
Soluble vascular cell adhesion molecules (sVCAM)
Soluble intercellular adhesion molecules (sICAM)
E-Selectin
Oxidised low-density lipoprotein
Myeloperoxidase
MicroRNA signatures for arterial, renal and retinal complications
Telomerase
DNA methylation/acetylation
GlycoMark
Isoprostanes and proteomics
Clotting profile
Methods
This is a multicentre, unblinded, parallel, randomised controlled phase III home trial, conducted by five tertiary paediatric diabetes centres in Australia. The trial has been approved. Ethics approval for the other four sites (The Children’s Hospital at Westmead, Sydney, John Hunter Children’s Hospital, Newcastle, Royal Children’s Hospital, Melbourne, and Women’s and Children’s Hospital, Adelaide are covered by a National Ethics Application at the Women’s and Children’s Hospital (HREC/16/WCHN/100). The trial is prospectively registered with the Australian New Zealand Clinic Trials Registry (ACTRN12616000753459). Inclusion and exclusion criteria are summarised in table 2.
Inclusion and exclusion criteria
Patient involvement
This study concept is a product of ongoing consumer engagement at the lead site (Princess Margaret Hospital) where the patients have advocated for the acceleration of automated insulin delivery systems. On a higher level, the Juvenile Diabetes Research Foundation (JDRF), which represents the T1D community have also called for research into these systems. The consumer engagement group at Princess Margaret Hospital (Perth) and JDRF were consulted throughout the study protocol development, and hence assessed the burden of the intervention. Study results will be disseminated through open participant and community forums, lay and scientific presentations and in scientific journals.
We will study adolescents and young adults aged 12–<25 years as this is a time that glycaemic control often deteriorates,6 highlighting the need for new treatment strategies. With an upper HbA1c cut-off of 10.5% (91mmol/mol), we will exclude participants who are less likely to comply and adhere to the protocol. Participants are approached through multiple avenues including directly in clinic, email and phone recruitment and through online advertising. Written informed consent is obtained from participants aged ≥18 years, and written parental consent and participant assent for those <18 years. Consent is attained by the research nurse. A participant may decide to withdraw from the study at any time without impacting future care. Once enrolled, the study duration is approximately 7 months, including a 4–5-week run-in, and 26-week study phase from randomisation.
To estimate the total sample size, data from the JDRF CGM randomised controlled trial were used.16 In this study, there were 97 subjects aged 12–<25 years who used injections or pumps at enrolment, and had a baseline HbA1c value <10.5%; participants were randomised to the control group (usual care), and had blinded CGM data at randomisation and at 6 months. The effective SD (after adjusting for baseline) was 13%. Assuming parallel groups, normal distribution for the treatment effect, a 1:1 allocation, a two-tailed test with null hypothesis stating that the difference is zero, no corrections for multiple comparisons, and a type I error=5%, 158 participants are required to detect an absolute 7% difference, using an SD of 13%, and 85% power (allowing for 20% predicted dropout). Outpatient data from trials to date typically show an improvement of 10%–20% for time in target range12; however, our recruitment pool typically has better glucose control at baseline in comparison to these studies.
A data safety monitoring board (DSMB) will meet quarterly, who will define stopping rules as part of their mandate.
HCL system
The intervention arm will use the MiniMed 670G insulin pump, coupled with a fourth-generation glucose sensor and GST3C transmitter (defined as HCL during the trial). The closed-loop algorithm is contained in the MiniMed 670G insulin pump, using a modified PID model, with insulin feedback and additional safety features. The algorithm receives CGM data every 5 min, and a ‘basal rate’ insulin delivery is computed and adjusted every 5 min. Therefore, standard ‘basal’ insulin that is preprogrammed in regular insulin pump therapy is replaced by the algorithm-derived insulin delivery (given as a microbolus every 5 min). When the algorithm is controlling insulin delivery, it is termed ‘Auto Mode’. Meals will still be announced, and an insulin bolus delivered according to the individualised patient carbohydrate ratio and insulin sensitivity factor (should a correction bolus be required in addition to the insulin for carbohydrate).
Blinded CGM will be collected three times during the study (baseline: at visit 3 for 3 weeks, midpoint: prior to visit 11 for 2 weeks, and prior to end for 3 weeks). A fourth-generation sensor will be inserted and a GST3C transmitter connected. Participants will be required to record finger prick glucose levels at least twice a day. CGM data are collected by uploading the GST3C and finger prick values from the CONTOUR NEXT LINK 2.4 from Bayer.
All participants will be issued with the CONTOUR NEXT LINK 2.4 from Bayer. This glucose monitor requires CONTOUR PLUS test strips. For participants randomised to HCL, this allows for data to be directly sent to the insulin pump. For participants not on HCL, the CONTOUR NEXT LINK 2.4 will be used in addition to their regular metre during CGM collection.
Carelink is a Medtronic web-based platform which is used for uploading insulin pump data. The Medtronic 670G can be uploaded, using the CONTOUR NEXT LINK 2.4, which is plugged into the Universal Serial Bus port of a personal computer. The software is Apple and Windows compatible. Insulin pump data are then accessible for download by the investigators.
Study protocol
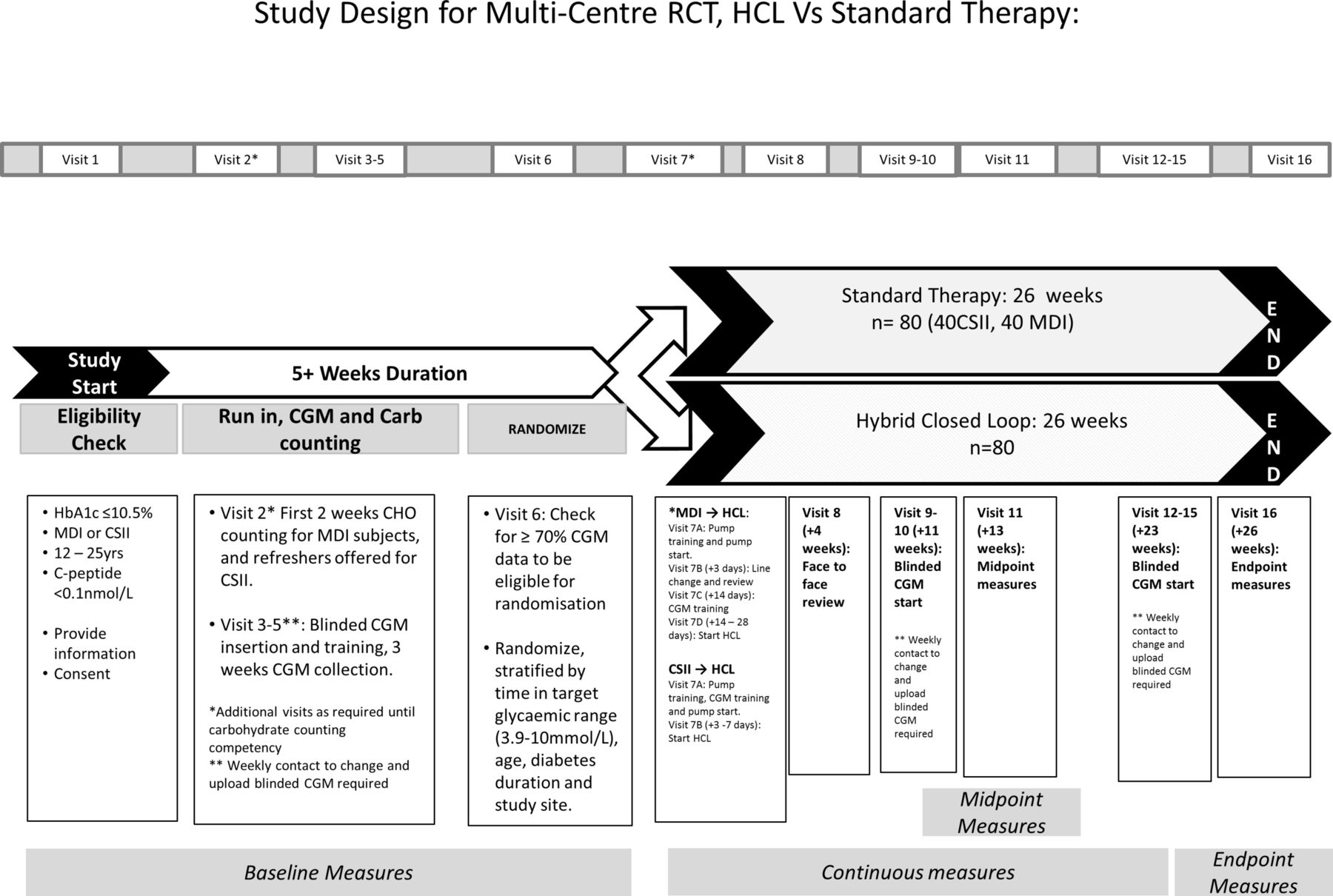
The study protocol is illustrated in schematic form in figure 1.
{kind=link}
Schematic outline of study. CGM, continuous glucose monitor; CHO, carbohydrate; HbA1c, haemoglobin A1c; HCL, hybrid closed loop; MDI, multiple daily injections; RCT, randomised controlled trial.
Visit 1 to visit 5 encompasses the run-in period which is 4 to 5 weeks in duration. Visit 1 is used to confirm eligibility for entry into the study, and for recording demographic (age, date of birth), auxological (height, weight) and clinical (date of diagnosis, HbA1c, current treatment regimen and insulin pump settings if applicable, blood pressure) data. A series of age-appropriate psychological questionnaires will be administered via an online platform (Qualtrics). The validated questionnaires and the frequency of administration are listed in table 3.
Questionnaires administered during the trial.
Visit 2 functions as an education review and supplemental visits may be required depending on the level of prior knowledge. Specifically, carbohydrate counting is reviewed until deemed competent by a dietitian, before visit 3 can occur. This is to ensure that all participants have the capability to operate HCL if randomised to the intervention. Visits 3 to 5 are scheduled visits to capture 3 weeks of baseline CGM data for the primary outcome. Participants will be issued with a logbook to record symptomatic hypoglycaemia and time off work by parents or school/work for participants. This diary will be kept for the duration of the trial.
Randomisation
At visit 6, participants will be randomised to HCL, or continue on their current treatment regimen. Participants will be allocated using minimisation with the following balancing factors: time in target glucose range (above or below 55%), sex, age, duration of diabetes and trial site. Participant randomisation is conducted by an independent third party (National Health and Medical Research Council Clinical Trials Centre, Sydney). Minimisation is a method of ensuring excellent balance between groups for known prognostic factors17; further detail on the minimisation process can be found elsewhere.18 Allocation concealment in this multisite study is protected through the centralised management of participant allocation by an independent third party: recruiters at each site do not have access to pooled strata information used in the minimisation process; their access is restricted to their site participants, protecting allocation concealment and reducing the predictability of allocations. While the study manager has access to the pooled data, this individual is separate from the randomisation process. Auxological and clinical parameters are recorded. Additionally, a fasting blood sample for biomarkers will be drawn. The list of biomarkers taken at visits 6 and 16 are listed in table 3. Participant flow for the rest of the trial is dependent on which group they are randomised to, and what baseline treatment regimen they were on.
Participants on MDI and CSII at baseline randomised to continue with standard therapy will have a face-to-face review at 4 weeks post randomisation for clinical review (visit 8). Two weeks of masked CGM collection will occur from 11 weeks post randomisation (visits 9 and 10). Repeat collection of auxological and clinical data as well as questionnaires occurs at the midpoint of the study, 13 weeks post randomisation (visit 11). At 23 weeks post randomisation, a final 3 weeks of masked CGM will be collected (visits 12, 13 and 14). The study ends after 26 weeks, with repeat collection of auxological and clinical data, as well as questionnaires, and biomarkers.
Participants on MDI randomised to HCL have education on CSII (visit 7A), will return for an observed line change 3 days later (visit 7B), receive CGM training 2 weeks after using the insulin pump (visit 7C) and, after a minimum of 3 days using SAP therapy, will be trained on and initiate Auto Mode (7D). Thereafter, visit 8 to visit 16 have the same assessments as those randomised to remain on standard therapy.
Participants on CSII randomised to HCL are trained on using the HCL system (visit 7A), and CGM. After a minimum of 3 days, the participant will be trained on and initiate Auto Mode (visit 7B). Thereafter, all visits are the same as for those randomised to standard therapy.
Participants who are using CGM as part of their standard therapy, or as part of the HCL system will need to wear a second masked CGM for consistency during the masked CGM collection phases.
From randomisation (visit 6), all participants will have an application installed on their smart phone (if available) for repeated sampling (weekly) of participant experiences of various aspects of daily living, including exercise, sleep, socialising, food and HCL-specific responses directed at trust and usability. The series of questions takes less than 1 min to respond on a Likert scale. A similar application with a different set of questions will assess experiences and expectations of HCL in healthcare professionals involved in the trial.
A subset of participants at the primary site (Princess Margaret Hospital) will be approached for a semistructured interview after the study is complete.
Data management and monitoring
Once enrolled, participants will be allocated a unique identifying number. A centralised database, managed at Princess Margaret Hospital, will collate all data input from study visits, questionnaires, insulin pumps, CGM and the mobile application with weekly sampling. The database will be kept on a secure server, with password protection.
A DSMB will be appointed for data review. Adverse events are defined as any undesirable clinical occurrence in a subject, whether it is considered to be device related or not, that includes a clinical sign, symptom or condition and/or an observation of an unintended technical performance or performance outcome of the device, and will be evaluated by the local investigator. A serious adverse event is defined as one which is fatal or life threatening or requires hospitalisation, including diabetic ketoacidosis or severe hypoglycaemia. All adverse and severe adverse events will be reported to the DSMB and relevant ethics committee. The DSMB will provide oversight for this study, and the aligned adult study. The following stopping rules will be adhered to: (1) Systematic hardware failure compromising participant safety, for example, recurrent diabetic ketoacidosis or injury, (2) systematic algorithm-driven severe hypoglycaemia and (3) greater than 50% post randomisation dropout.
Statistical analysis
A detailed statistical analysis plan will be reported elsewhere and, here, we describe the approach for the primary outcome only. All statistical analyses will be performed using SAS for Windows (SAS Institute) and STATA (StataCorp). The analysis population will be the intention-to-treat (ITT) population, which will be defined as all participants who are randomised and have at least one visit after baseline. P values <0.05 will be considered statistically significant and two-sided p values will be reported. Descriptive statistics will be used to characterise participants at study entry.
The primary endpoint, average % time spent in target glucose range (sensor glucose level 3.9–10.0 mmol/L) during the final 3-week blinded sensor period, will be analysed using analysis of covariance (ANCOVA) adjusting for baseline percentage score. Least square means and least square mean differences and their associated 95% CI will be presented for each treatment group and between groups. In the event that residuals are not normally distributed: the Mann-Whitney-Wilcoxon (Wilcoxon rank sum) test will be employed if raw data are symmetric; if raw data are non-symmetric, bootstrap methods19 will be used to test the difference in means. Multiple imputation will be used to deal with missing data in the ITT analysis.
Continuous secondary outcomes will be analysed using ANCOVA adjusting for baseline values, count outcomes will be analysed using Poisson regression (or negative binomial regression where overdispersion is apparent) and logistic regression will be used for binomial outcomes. Non-parametric methods will be used where model fit is poor and transformations are unsuccessful. Subgroup analysis by baseline insulin regimen will be performed by including an interaction term in the regression modelling, whereas where non-parametric methods are used, subgroup analysis will be performed by stratifying by baseline insulin regimen.
A separate economic analysis will be conducted using costs (resource units) and measures of functional health status (using the EuroQuol-5 Dimension-Youth (EQ-5D)) collected during the trial to estimate incremental cost-effectiveness of automated insulin delivery compared with standard treatment. A health economics protocol will be published independently as this paper is focused on the primary outcome.
No corrections for multiplicity are planned; rather, a transparent approach to reporting results will be taken, with all effects, CI and p values for the primary and secondary outcomes being presented.20
Discussion
HCL is an important advancement in the management of T1D, and has potential to improve glycaemic and quality of life outcomes. There are several international multicentre randomised outpatient trials investigating the efficacy and safety of automated insulin delivery currently underway (as registered at https://clinicaltrials.gov). The point of difference of this study (and the aligned adult study) is that these are the first studies to compare HCL with standard care—including participants using MDI and CSII, with or without adjunctive CGM. The justification for a heterogeneous standard care control arm is that this study will provide comparative data for all people with T1D when considering the option of using HCL. By representing the diverse treatment options that are currently in use by people with T1D, the data from the study will better inform the role of HCL in the general T1D clinic, allowing clinicians and patients to make evidence-based decisions. Careful attention to education in the run-in phase will reduce the possible bias created by potential unequal contact time with research staff favouring participants randomised to HCL. This will add strength to the planned health economic evaluation which in turn will inform funding decisions to facilitate access to these technologies in the future. The inclusion of MDI as a comparative arm in diabetes technology studies has precedent.21 This study in those aged 12–<25 years is complemented by a parallel study being conducted in seven adult centres across Australia in people aged greater than 25 years with T1D.
Acknowledgments
The protocol was reviewed by a protocol optimisation committee that included representation from the Jaeb Center for Health Research and Cambridge University (Roy Beck, Roman Hovorka).
References
Footnotes
Contributors MB, SAM, MBA and JN contributed to the study design and were responsible for writing the detailed protocol. TWJ, EAD and DNO were responsible for study concept and design and provided expert opinion and oversight during protocol development. GS provided statistical analyses input. EAG provided input to the protocol that will inform health economic data. GRA, FJC, JMF and BRK reviewed and refined the study protocol to ensure feasibility at the non-lead sites.
Funding The study is supported by Juvenile Diabetes Research Foundation (JDRF) Australia, the recipient of the Australia Research Council Special Research Initiative in Type 1 Juvenile Diabetes. MDB was funded by Western Australia Department of Health and the Raine Medical Research Foundation, and the Australian Type 1 Diabetes Clinical Research Network initiative undertaken by the JDRF Australia supported by funding from the Australian Government Department of Health and Ageing. SAM is supported by a JDRF Early-Career Patient-Orientated Diabetes Research Award. Insulin pumps, transmitter and glucose sensors were provided by Medtronic via an unrestricted grant. MA was supported by JDRF Australia, the recipient of the Australian Research Council Special Research Initiative in Type 1 Juvenile Diabetes.
Disclaimer Medtronic has no role in the design and conduct of the study; data collection, analysis and interpretation of the data; the preparation, review or approval of the manuscript; and decision to submit the manuscript.
Competing interests MB reports receiving speaker honoraria from Medtronic. DNO reports receiving speaker honoraria and research grants from Medtronic.
Patient consent Not required.
Ethics approval Princess Margaret Hospital Ethics Committee Perth(HREC/2016087EP).
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators Leon A Bach; Morton G Burt; Philip M Clarke; Neale D Cohen; Peter G Colman; Christel Hendrieckx; D Jane Holmes-Walker; Jodie C Horsburgh; Alicia J Jenkins; Joey Kaye; Anthony C Keech; Kavita Kumareswaran; Melissa H Lee; Richard J MacIsaac; Roland W McCallum; Barbora Paldus; Catriona Sims; Jane Speight; Stephen N Stranks; Vijaya Sundararajan; Steven Trawley; Sara Vogrin; Glenn M Ward.