
Progress towards Achieving the Recommendations of the Commission on Ending Childhood Obesity: A Comprehensive Review and Analysis of Current Policies, Actions and Implementation Gaps in Thailand


Abstract
:1. Introduction
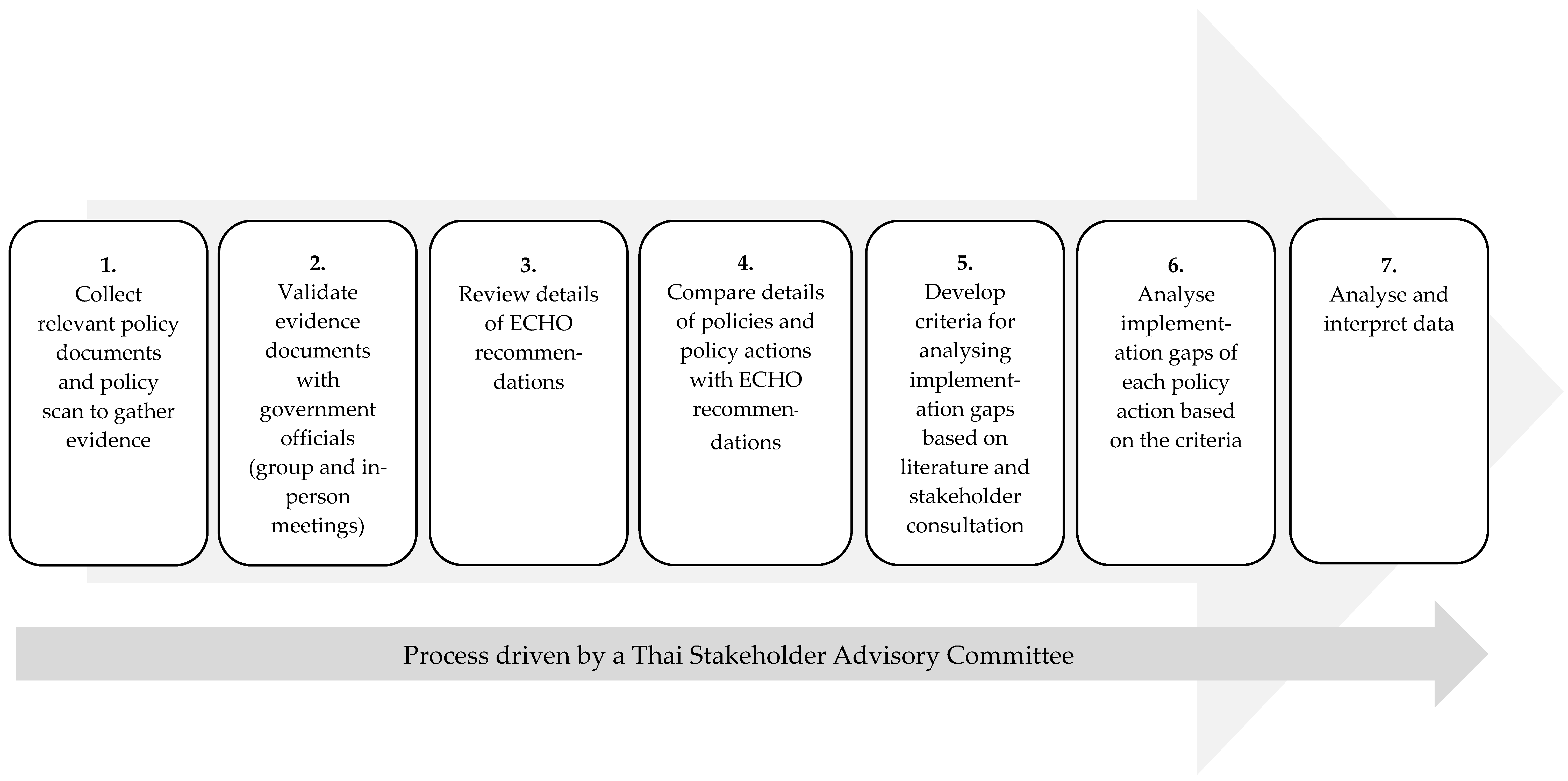
2. Materials and Methods
2.1. Data Collection and Verification
Document Assessment
2.2. Data Analysis
2.3. Preparation of Recommendations
3. Results
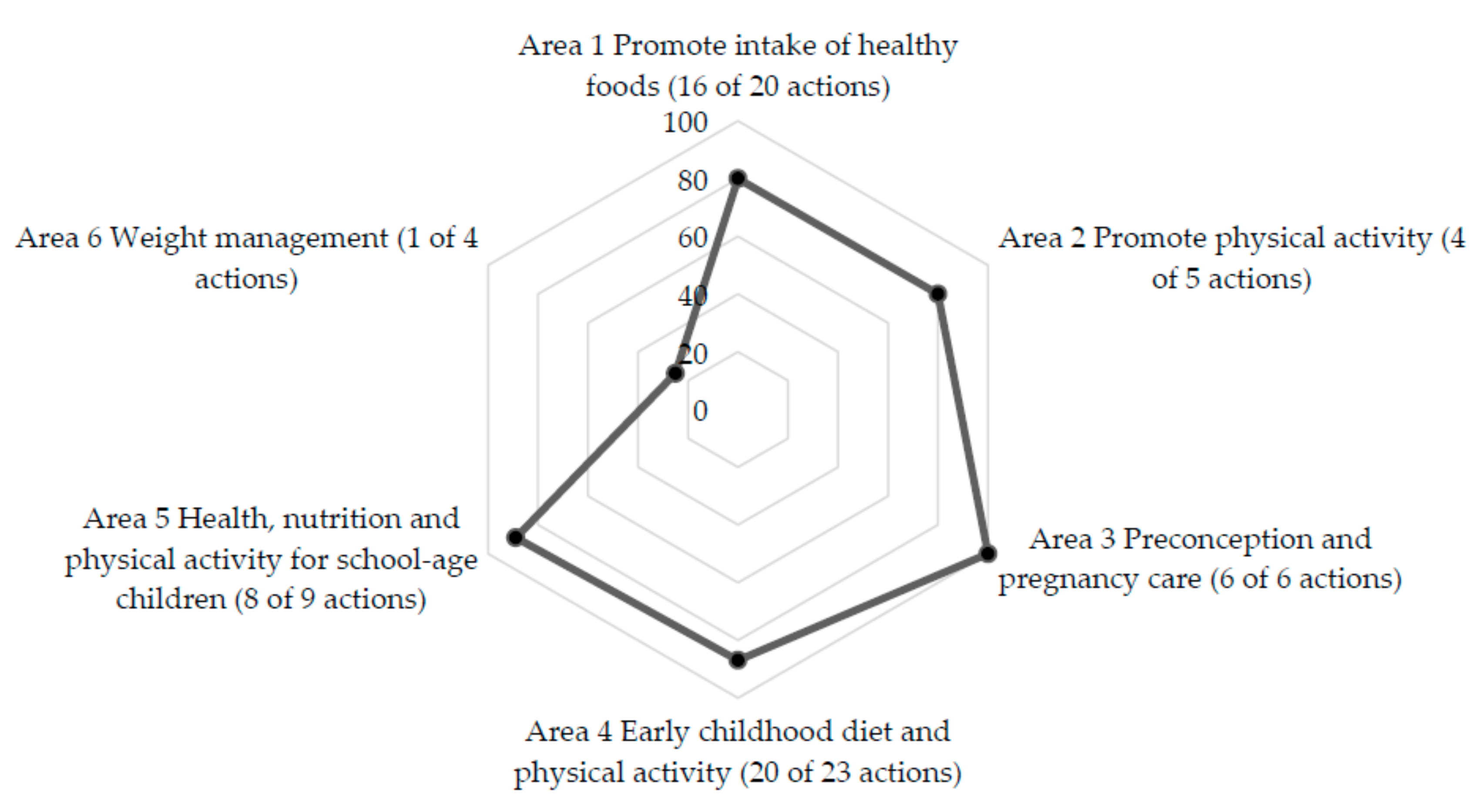
3.1. Government Policy Implementation against ECHO Recommendations
3.2. Identification of Policy Implementation Gaps
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 1 April 2020).
- World Health Organization. Report of the Commission on Ending Childhood Obesity; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. Report of the Commission on Ending Childhood Obesity. Implementation Plan: Executive Summary; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Swinburn, B.; Vandevijvere, S. WHO report on ending childhood obesity echoes earlier recommendations. Public Health Nutr. 2016, 19, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esdaile, E.; Thow, A.M.; Gill, T.; Sacks, G.; Golley, R.; Love, P.; Wen, L.M.; Rissel, C. National policies to prevent obesity in early childhood: Using policy mapping to compare policy lessons for Australia with six developed countries. Obes. Rev. 2019, 20, 1542–1556. [Google Scholar] [CrossRef] [PubMed]
- Ezzeddin, N.; Eini-Zinab, H.; Ajami, M.; Kalantari, N.; Sheikhi, M. WHO Ending Childhood Obesity and Iran-Ending Childhood Obesity Programs based on urban health equity indicators: A qualitative content analysis. Arch. Iran Med. 2019, 22, 646–652. [Google Scholar] [PubMed]
- Development Initiatives. Thailand-Global Nutrition Report Bristol, UK: Development Initiatives. Available online: https://globalnutritionreport.org/resources/nutrition-profiles/asia/south-eastern-asia/thailand/ (accessed on 4 January 2021).
- Prakongsai, P.; Limwattananon, S.; Tangcharoensathien, V. The equity impact of the universal coverage policy: Lessons from Thailand. In Innovations in Health System Finance in Developing and Transitional Economies; Chernichovsky, D., Hanson, K., Eds.; Emerald: Bingley, UK, 2009. [Google Scholar]
- Aekplakorn, W.; Porapakam, Y.; Taneepanichskul, S.; Puckcharern, H.; Satheannoppakao, W.; Thaigla, K. Report on the Forth National Health Examination Survey (2008-9); National Health Examination Survey Office and Health System Research Institute: Nonthaburi, Thailand, 2011. [Google Scholar]
- Aekplakorn, W.; Puckcharern, H.; Thaigla, K.; Satheannoppakao, W. Report on the Fifth National Health Examination Survey (2014); Institute, H.S.R., Ed.; Health System Research Institute, Ministry of Public Health and Thai Health Promotion Foundation: Nonthaburi, Thailand, 2016. [Google Scholar]
- Mo-suwan, L. Holistic Development of Thai Children Project; Prince of Songkla University: Hat Yai, Thailand, 2001. [Google Scholar]
- Second National Health Examination Survey Working Group. Report on the Second National Health Examination Survey (1996); National Health Foundation and Minstry of Public Health: Bangkok, Thailand, 1998. [Google Scholar]
- Department of Health. Implementation Plan for the Miracle of 1,000 Days Policy; Department of Health, Ministry of Public Health Thailand: Nonthaburi, Thailand, 2018.
- Osornprasop, S.; Phulkerd, S.; Gowachirapant, S. Lessons Learned from Thailand's Obesity Prevention and Control Policies; World Bank Group: Washington, DC, USA, 2018. [Google Scholar]
- National Strategy Secretariat Office; Office of the National Economic and Social Development Council. National Strategy 2018–2037; Government of Thailand: Bangkok, Thailand, 2018; pp. 1–74.
- Office of the National Economic and Social Development Board. Summary. In The Twelfth National Economic and Social Development Plan; Office of the National Economic and Social Development Board, Ed.; Office of the National Economic and Social Development Board, Office of the Prime Minister: Bangkok, Thailand, 2017. [Google Scholar]
- Bureau of Nutrition. Meeting Report on Implementing Key Performance Indicators for the Fiscal Year 2020 Nonthaburi: Bureau of Nutrition, Department of Health. Available online: https://nutrition.anamai.moph.go.th/main.php?filename=report_new (accessed on 1 February 2021).
- Bureau of Nutrition. The Five-Year National Nutrition Action Plan; Bureau of Nutrition, Department of Health, Ministry of Public Health Thailand: Nonthaburi, Thailand, 2018.
- Topothai, T.; Khamput, T.; Kamonrungsan, J.; Promsaka Na Sakolnakorn, P.; Asawutmangkul, U. Lessons Learnt from Developing the 2018–2030 National Physical Activity Plan in Thailand. J. Health Syst. Res. 2019, 13, 442–456. [Google Scholar]
- Thai Health Promotion Foundation. Physical Activity. Available online: https://resourcecenter.thaihealth.or.th/index.php/media/list?keyword=%E0%B8%81%E0%B8%B4%E0%B8%88%E0%B8%81%E0%B8%A3%E0%B8%A3%E0%B8%A1%E0%B8%97%E0%B8%B2%E0%B8%87%E0%B8%81%E0%B8%B2%E0%B8%A2&issue=0&template=0&target=0 (accessed on 23 May 2021).
- Phulkerd, S.; Vandevijvere, S.; Lawrence, M.; Tangcharoensathien, V.; Sacks, G. Level of implementation of best practice policies for creating healthy food environments: Assessment by state and non-state actors in Thailand. Public Health Nutr. 2017, 20, 381–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyaaba, G.N.; Stronks, K.; Masana, L.; Larrea-Killinger, C.; Agyemang, C. Implementing a national non-communicable disease policy in sub-Saharan Africa: Experiences of key stakeholders in Ghana. Health Policy OPEN 2020, 1, 100009. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe. Country Experiences in Integrated Policy Development for the Prevention and Control of Noncommunicable Diseases; WHO Regional Office for Europe: Copenhagen, Denmark, 2015. [Google Scholar]
- Musango, L.; Timol, M.; Burhoo, P.; Shaikh, F.; Donnen, P.; Kirigia, J.M. Assessing health system challenges and opportunities for better noncommunicable disease outcomes: The case of Mauritius. BMC Health Serv. Res. 2020, 20, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juma, P.A.; Mapa-tassou, C.; Mohamed, S.F.; Matanje Mwagomba, B.L.; Ndinda, C.; Oluwasanu, M.; Mbanya, J.-C.; Nkhata, M.J.; Asiki, G.; Kyobutungi, C. Multi-sectoral action in non-communicable disease prevention policy development in five African countries. BMC Public Health 2018, 18, 953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuangratananon, T.; Wangmo, S.; Widanapathirana, N.; Pongutta, S.; Viriyathorn, S.; Patcharanarumol, W.; Thin, K.; Nagpal, S.; Nuevo, C.E.L.; Padmawati, R.S.; et al. Implementation of national action plans on noncommunicable diseases, Bhutan, Cambodia, Indonesia, Philippines, Sri Lanka, Thailand and Viet Nam. Bull. World Health Organ. 2019, 97, 129–141. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.M.; Unwin, N.; Samuels, T.A.; Hassel, T.A.; Bishop, L.; Guell, C. Evaluating policy responses to noncommunicable diseases in seven Caribbean countries: Challenges to addressing unhealthy diets and physical inactivity. Rev. Panam. Salud Publica 2018, 42, 174. [Google Scholar] [CrossRef] [PubMed]
- WHO Regional Office for Europe. Policy Coherence as A Driver of Health Equity; WHO Regional Office for Europe: Copenhagen, Denmark, 2019. [Google Scholar]
- OECD. Better Policies for Development 2015: Policy Coherence and Green Growth; OECD: Paris, France, 2015. [Google Scholar]
- Collins, T.E.; Nugent, R.; Webb, D.; Placella, E.; Evans, T.; Akinnawo, A. Time to align: Development cooperation for the prevention and control of non-communicable diseases. BMJ 2019, 366, l4499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Topothai, C.; Chaweewan, T. Maternal and Child Health: Benefit Package under the Thai Universal Health Coverage; Japan International Cooperation Agency: Nonthaburi, Thailand, 2018. [Google Scholar]
- Limwattananon, S.; Tangcharoensathien, V.; Prakongsai, P. Equity in maternal and child health in Thailand. Bull. World Health Organ. 2010, 88, 420–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, B.; Miller, R.; King, L. The case for and against the regulation of food marketing directed towards children. In A Modern Epidemic: Expert Perspectives on Obesity and Diabetes; Baur, L., Twigg, S.M., Magnusson, R.S., Eds.; Sydney University Press: Sydney, Australia, 2012; pp. 129–145. [Google Scholar]
- The Advertising Association of Thailand. Thailand Childrens Food and Beverage Advertising Initiative 2008. Available online: https://issuu.com/foodindustryclub/stacks/5d53361f66454db6a6f71292878b89d4 (accessed on 28 January 2021).
- Jaichuen, N. Digital Television: Food Advertising to Children in Thailand; Food and Nutrition Policy for Health Promotion Program: Nonthaburi, Thailand, 2015. [Google Scholar]
- WHO Regional Office for Europe. Evaluating Implementation of the WHO Set of Recommendations on the Marketing of Foods and Non-alcoholic Beverages to Children; WHO Regional Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]
- WHO Regional Office for Europe. Prevention and Control of Noncommunicable Diseases in the European Region: A Progress Report; WHO Regional Office for Europe: Copenhagen, Denmark, 2014. [Google Scholar]
- Thow, A.M.; Greenberg, S.; Hara, M.; Friel, S.; duToit, A.; Sanders, D. Improving policy coherence for food security and nutrition in South Africa: A qualitative policy analysis. Food Secur. 2018, 10, 1105–1130. [Google Scholar] [CrossRef] [Green Version]
- Dodd, R.; Reeve, E.; Sparks, E.; George, A.; Vivili, P.; Win Tin, S.T.; Buresova, D.; Webster, J.; Thow, A.-M. The politics of food in the Pacific: Coherence and tension in regional policies on nutrition, the food environment and non-communicable diseases. Public Health Nutr. 2020, 23, 168–180. [Google Scholar] [CrossRef] [PubMed]
- Kusek, J.Z.; Rist, R.C. Ten Steps to A Results-Based Monitoring and Evaluation System; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2004. [Google Scholar]
- Liberali, R.; Kupek, E.; Assis, M.A.A. Dietary patterns and childhood obesity risk: A systematic review. Child. Obes. 2020, 16, 70–85. [Google Scholar] [CrossRef] [PubMed]
- Ambrosini, G.L. Childhood dietary patterns and later obesity: A review of the evidence. Proc. Nutr. Soc. 2013, 73, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.; Milton, K.; Kahlmeier, S. Health-Enhancing Physical Activity (HEPA) Policy Audit Tool (PAT); Version 2; WHO Regional Office for Europe: Copenhagen, Denmark, 2015. [Google Scholar]
- Swinburn, B.; Vandevijvere, S.; Kraak, V.; Sacks, G.; Snowdon, W.; Hawkes, C.; Barquera, S.; Friel, S.; Kelly, B.; Kumanyika, S.; et al. Monitoring and benchmarking government policies and actions to improve the healthiness of food environments: A proposed Government Healthy Food Environment Policy Index. Obes. Rev. 2013, 14, 24–37. [Google Scholar] [CrossRef] [PubMed]
- Sacks, G.; Vanderlee, L.; Robinson, E.; Vandevijvere, S.; Cameron, A.J.; Ni Mhurchu, C.; Lee, A.; Ng, S.H.; Karupaiah, T.; Vergeer, L.; et al. BIA-Obesity (Business Impact Assessment—Obesity and population-level nutrition): A tool and process to assess food company policies and commitments related to obesity prevention and population nutrition at the national level. Obes. Rev. 2019, 20, 78–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Criteria | Description of Each Criterion | Rating Scale (Performance Level and Definition) |
|---|---|---|
| Refers to elements of ECHO that are contained in the policy content. |
|
| Refers to a level that a policy/action can reach target group/setting. |
|
| Refers to the availability of monitoring and process and outcome evaluation plan in each policy/action. |
|
| Refers to the level of collaboration between organizations in different areas of policy (e.g., health, social, environment) and different sectors (e.g., public, private, third), as well as communities and people, working together to achieve policy outcomes. |
|
| Refers to the definition of OECD [29] which is the creation of a systematic promotion of mutually reinforcing policy actions across government departments and agencies creating synergies towards achieving the agreed objectives. |
|
| ECHO Recommendations | Thailand's Implementation Based on ECHO Recommendations | Overall Assessment of Thailand Implementation | ||
|---|---|---|---|---|
| Policy Area | Broad Policy Action | Specific Policy Action | ||
| Area 1 Promote intake of healthy foods | 1.1 Appropriate and context-specific nutrition information and guidelines | 1.1.1 | ✓ | L |
| 1.1.2 | ✓ | L | ||
| 1.1.3 | ✓ | M | ||
| 1.1.4 | ✓ | L | ||
| 1.2 An effective tax on sugar-sweetened beverages. | 1.2.1 | ✓ | M | |
| 1.2.2 | ✓ | H | ||
| 1.3 The set of recommendations on the marketing of foods and non-alcoholic beverages to children | 1.3.1 | NA | NA | |
| 1.3.2 | NA | NA | ||
| 1.3.3 | NA | NA | ||
| 1.4 Nutrient profiles to identify unhealthy foods and beverages | 1.4.1 | ✓ | L | |
| 1.5 Impact of cross-border marketing of unhealthy foods and beverages | 1.5.1 | NA | NA | |
| 1.6 A standardized global nutrient-labeling system | 1.6.1 | ✓ | M | |
| 1.6.2 | ✓ | H | ||
| 1.7 Interpretive front-of-pack labeling | 1.7.1 | ✓ | M | |
| 1.7.2 | ✓ | M | ||
| 1.8 Healthy food environments in child settings | 1.8.1 | ✓ | M | |
| 1.8.2 | ✓ | M | ||
| 1.9 Access to healthy foods in disadvantaged communities | 1.9.1 | ✓ | L | |
| 1.9.2 | ✓ | L | ||
| 1.9.3 | ✓ | L | ||
| Area 2 Promote physical activity | 2.1 Guidance to children and adolescents, their parents, carers, teachers and health professionals | 2.1.1 | ✓ | L |
| 2.1.2 | ✓ | L | ||
| 2.1.3 | ✓ | L | ||
| 2.1.4 | NA | NA | ||
| 2.2 Facilities on school premises and in public spaces for physical activity during recreational time | 2.2.1 | ✓ | M | |
| Area 3 Preconception and pregnancy care | 3.1 Diagnosis and management of hyperglycemia and gestational hypertension | 3.1.1 | ✓ | M |
| 3.2 Monitoring and management of gestational weight gain | 3.2.1 | ✓ | M | |
| 3.3 Appropriate nutrition in guidance and advice | - | ✓ | H | |
| 3.4 Guidance and support for the promotion of good nutrition, healthy diets and physical activity | 3.4.1 | ✓ | M | |
| 3.4.2 | ✓ | M | ||
| 3.4.3 | ✓ | M | ||
| Area 4 Early childhood diet and physical activity | 4.1 Regulatory measures such as the International Code of Marketing of Breast-milk Substitutes | - | ✓ | H |
| 4.2 A full practice for the Ten Steps to Successful Breastfeeding | - | ✓ | M | |
| 4.3 Promotion of the benefits of breastfeeding for both mother and child | - | ✓ | L | |
| 4.4 Regulatory measures for supporting maternal breastfeeding | 4.4.1 | ✓ | H | |
| 4.5 Regulations on the marketing of complementary foods and beverages | 4.5.1 | NA | NA | |
| 4.5.2 | ✓ | H | ||
| 4.5.3 | ✓ | H | ||
| 4.6 Guidance and support to carers to avoid specific categories of foods | - | ✓ | M | |
| 4.7 Guidance and support to caregivers to encourage the consumption of a wide variety of healthy foods | - | ✓ | M | |
| 4.8 Guidance to caregivers on appropriate nutrition, diet and portion size | 4.8.1 | ✓ | M | |
| 4.8.2 | ✓ | M | ||
| 4.9 Provision of healthy foods, beverages and snacks in formal child-care settings | 4.9.1 | ✓ | L | |
| 4.9.2 | ✓ | L | ||
| 4.10 Food education in the curriculum in formal child-care settings | 4.10.1 | NA | NA | |
| 4.10.2 | NA | NA | ||
| 4.11 Physical activity in the daily routine and curriculum in formal childcare settings | 4.11.1 | ✓ | L | |
| 4.11.2 | ✓ | L | ||
| 4.12 Guidance on appropriate sleep time, sedentary or screen-time, and physical activity or active play | 4.12.1 | ✓ | L | |
| 4.12.2 | ✓ | L | ||
| 4.13 Whole-of-community support for carers and child-care settings | 4.13.1 | ✓ | M | |
| 4.13.2 | ✓ | M | ||
| 4.13.3 | ✓ | M | ||
| 4.13.4 | ✓ | M | ||
| Area 5 Health, nutrition and physical activity for school-age children | 5.1 Standards for meals provided in schools, or foods and beverages sold in schools | - | ✓ | M |
| 5.2 Elimination of provision or sale of unhealthy foods | 5.2.1 | ✓ | L | |
| 5.2.2 | ✓ | L | ||
| 5.3 Access to potable water in schools and sports facilities | 5.3.1 | ✓ | L | |
| 5.4 Inclusion of nutrition and health education within the core curriculum of schools | 5.4.1 | NA | NA | |
| 5.4.2 | ✓ | L | ||
| 5.5 Nutrition literacy and skills of parents and carers. | - | ✓ | L | |
| 5.6 Food preparation classes to children, their parents and carers | 5.6.1 | ✓ | L | |
| 5.7 Physical education in the school curriculum | 5.7.1 | ✓ | M | |
| Area 6 Weight management of children with obesity | 6.1 Appropriate weight management services for children and adolescents with overweight or obesity | 6.1.1 | ✓ | L |
| 6.1.2 | NA | NA | ||
| 6.1.3 | NA | NA | ||
| 6.1.4 | NA | NA | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phulkerd, S.; Nakraksa, P.; Mo-suwan, L.; Lawrence, M. Progress towards Achieving the Recommendations of the Commission on Ending Childhood Obesity: A Comprehensive Review and Analysis of Current Policies, Actions and Implementation Gaps in Thailand. Nutrients 2021, 13, 1927. https://doi.org/10.3390/nu13061927
Phulkerd S, Nakraksa P, Mo-suwan L, Lawrence M. Progress towards Achieving the Recommendations of the Commission on Ending Childhood Obesity: A Comprehensive Review and Analysis of Current Policies, Actions and Implementation Gaps in Thailand. Nutrients. 2021; 13(6):1927. https://doi.org/10.3390/nu13061927
Chicago/Turabian StylePhulkerd, Sirinya, Parichat Nakraksa, Ladda Mo-suwan, and Mark Lawrence. 2021. "Progress towards Achieving the Recommendations of the Commission on Ending Childhood Obesity: A Comprehensive Review and Analysis of Current Policies, Actions and Implementation Gaps in Thailand" Nutrients 13, no. 6: 1927. https://doi.org/10.3390/nu13061927